Permanent Hemorrhoid Treatment: How to Treat Piles Permanently
-

- March 19th, 2026
- 354 views

Get a free topical map and start building content authority today.
Permanent hemorrhoid treatment is a realistic goal for many people when the correct combination of diagnosis, lifestyle changes, and procedural care is used. This guide explains how to treat piles permanently by weighing non-surgical therapies, minimally invasive procedures, and surgical options and showing how to choose the right plan for lasting results.
- Most lasting relief requires a clear diagnosis (internal vs external) and a targeted approach.
- Start with lifestyle, fiber, and medical treatments; escalate to office procedures (rubber band ligation, sclerotherapy) or surgery if needed.
- Permanent results are possible, but recurrence risk depends on patient factors and treatment choice.
Detected intent: Informational
Overview: What permanent hemorrhoid treatment means
Permanent hemorrhoid treatment refers to interventions that remove or remodel symptomatic hemorrhoidal tissue and reduce recurrence risk. Terms used interchangeably include piles treatment, hemorrhoid removal options, and long-term piles treatment. Accurate classification (internal, external, thrombosed) and symptom assessment guide whether conservative care, office procedures, or surgery is appropriate.
Permanent hemorrhoid treatment options
Treatment paths fall into three tiers: conservative management, office/minimally invasive procedures, and surgical interventions. Each tier has trade-offs in recovery time, effectiveness, and recurrence rates.
Conservative and medical measures
Dietary fiber, stool softeners, good anal hygiene, and weight or activity changes are the foundation. For many people these measures control symptoms and lower recurrence risk. Over-the-counter topical agents help short-term but do not produce permanent anatomical changes.
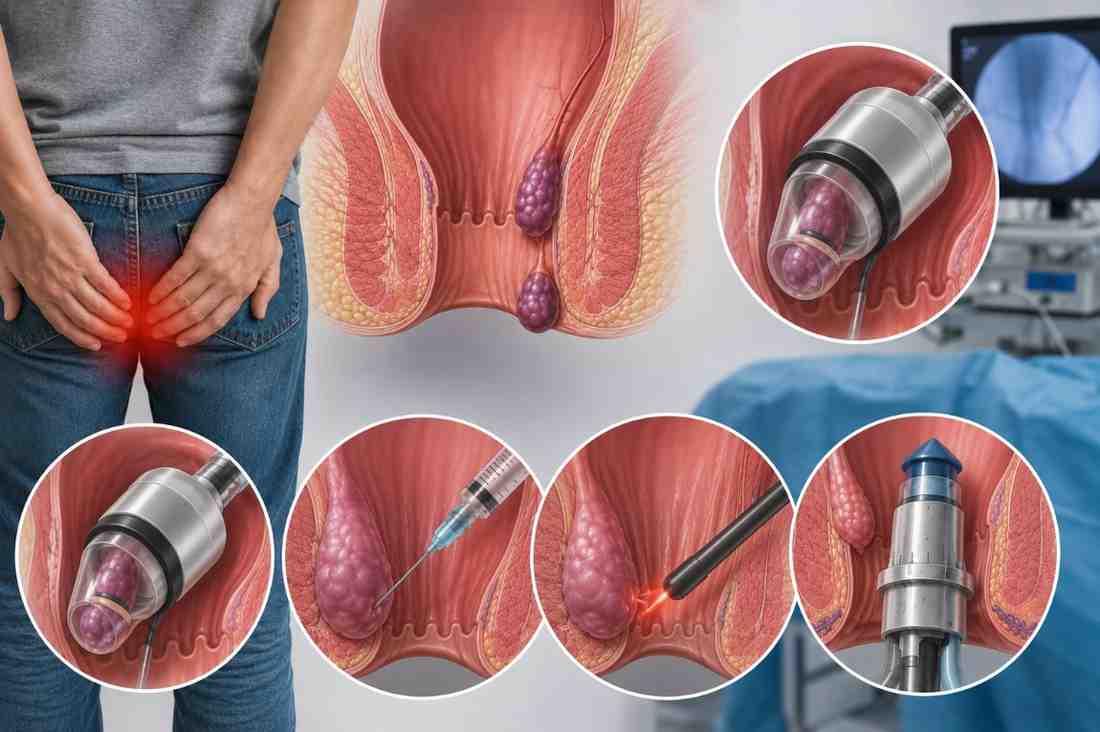
Office and minimally invasive procedures
Procedures such as rubber band ligation, sclerotherapy, and infrared coagulation remove or shrink internal hemorrhoids with minimal downtime. These are often used when conservative care fails and are grouped under hemorrhoid removal options that avoid full surgery.
Surgical options
Surgery—hemorrhoidectomy, stapled hemorrhoidopexy, or Doppler-guided ligation—provides the highest chance of durable symptom elimination for large or recurrent piles. Surgery has longer recovery and higher immediate pain but can be the most definitive approach for severe disease.
HEAL checklist: a named framework for planning treatment
- History & examination: confirm symptoms, bleeding, prolapse, pain.
- Evaluate options: conservative vs office procedures vs surgery.
- Assess risk factors: constipation, BMI, pregnancy, anticoagulants.
- Locate specialist & plan: colorectal surgeon or experienced proctologist and a stepwise treatment plan with follow-up.
Choosing between options: trade-offs and common mistakes
Trade-offs include recovery time vs permanence: office procedures have quicker recovery but slightly higher recurrence compared with surgical hemorrhoidectomy, which is more invasive but often more durable. Common mistakes include skipping a proper diagnosis, assuming home remedies will cure advanced prolapse, or delaying treatment until complications (thrombosis, severe bleeding) occur.
Short real-world example
Scenario: A 48-year-old with ongoing prolapse and intermittent bleeding tried fiber and topical creams for 8 months with partial relief. Diagnosis: Grade II–III internal hemorrhoids. Plan: rubber band ligation in clinic; two sessions over 6 weeks resolved prolapse and bleeding. After a 12‑month follow-up with dietary changes, symptoms remained controlled. This illustrates stepping up from conservative care to office procedures as an effective pathway toward long-term piles treatment.
Practical tips for lasting results
- Increase dietary fiber to 25–35 g/day and maintain 1.5–2 L of fluids daily to produce soft, formed stools.
- Adopt regular bowel habits—avoid straining and limit time on the toilet to reduce pressure on anal cushions.
- When symptoms persist after 4–6 weeks of conservative care, consult a specialist to consider office procedures rather than prolonged topical use.
- Discuss blood thinners, pregnancy plans, and chronic constipation with the clinician before choosing an invasive procedure.
Core cluster questions
- What are the most effective long-term treatments for internal hemorrhoids?
- How do rubber band ligation and hemorrhoidectomy compare for lasting relief?
- What lifestyle changes reduce the chance of piles returning?
- When should surgical hemorrhoid removal be considered?
- What are the recovery timelines and risks for different hemorrhoid procedures?
Choosing a provider and what to expect
Seek a colorectal surgeon or proctologist for Grade III–IV disease or recurrent symptoms. For milder disease, experienced general surgeons or GI practices offering office procedures are appropriate. Official clinical guidance and patient information pages can clarify procedure indications and recovery expectations: NHS—Haemorrhoids.
Common mistakes to avoid
- Relying solely on topical creams for advanced prolapse—delays definitive care and may worsen bleeding.
- Assuming all hemorrhoid procedures are equally invasive—treatment choice matters for recovery and recurrence.
- Neglecting follow-up and lifestyle measures after a procedure—prevention is part of permanent care.
FAQ
What is permanent hemorrhoid treatment and is it possible?
Permanent hemorrhoid treatment aims to remove or greatly reduce symptomatic hemorrhoidal tissue and lower recurrence. Procedures like hemorrhoidectomy have the highest long-term success rates, while office procedures and lifestyle changes can provide lasting relief for many patients. Success depends on disease severity and addressing contributing factors such as constipation.
How long is recovery after common hemorrhoid procedures?
Recovery varies: rubber band ligation and sclerotherapy usually allow return to normal activity within days; hemorrhoidectomy often requires 1–3 weeks for full recovery and pain management. Discuss pain control and wound care with the treating clinician.
Can lifestyle changes prevent hemorrhoids from coming back?
Yes. Increasing fiber, staying hydrated, avoiding straining, and maintaining healthy weight reduce pressure on anal cushions and lower the risk of recurrence after treatment.
Are there risks of permanent incontinence after surgery?
Major long-term continence problems are uncommon with modern techniques when performed by experienced surgeons, but risks depend on the procedure and patient factors. Detailed preoperative counseling should cover risks and expected outcomes.
When should a doctor be contacted urgently?
Seek urgent care for heavy bleeding, severe uncontrolled pain, fever, or signs of infection. Thrombosed external hemorrhoids with severe, sudden pain also warrant prompt evaluation.
This guide outlines pragmatic steps to treat piles permanently: start with clear diagnosis, proceed through a stepwise HEAL checklist, and combine effective procedures with lifestyle prevention to maximize the chance of long-term success.