Pelvic Girdle Pain Guide: Causes, Diagnosis, and Practical Treatments
-

- May 06th, 2026
- 637 views

FREE SEO Topical Map Generator: Find Your Next Content Ideas
Detected intent: Informational
pelvic girdle pain is a common condition that affects the joints and muscles around the pelvis and can limit walking, standing, and daily activities. This guide explains what it is, how it is diagnosed, practical self-management strategies, evidence-based treatments, and when to seek professional care.
- Pelvic girdle pain typically involves the sacroiliac joints, symphysis pubis, and surrounding ligaments and muscles.
- Assessment focuses on pain pattern, functional limitations, and movement tests; imaging is rarely required unless red flags exist.
- First-line management: education, graded activity, targeted exercise, pelvic support, and guided physical therapy.
- Most people improve with conservative care; persistent or severe cases may need multidisciplinary treatment.
pelvic girdle pain: Overview and key facts
Pelvic girdle pain describes discomfort originating from the bony pelvis and its supporting soft tissues. Common synonyms or related terms include sacroiliac joint pain, symphysis pubis dysfunction (SPD), and pelvic ring pain. Symptoms vary from a dull ache to sharp, stabbing pain with changes in posture, walking, climbing stairs, or turning in bed.
How pelvic girdle pain is diagnosed
Clinical assessment
Diagnosis is primarily clinical. Providers use a history and focused physical exam to identify pain provoked by pelvic movements, single-leg stance tests, and pain during straight-leg raise or palpation of the pubic symphysis. Functional questions—pain with dressing, rolling, standing on one leg—help target treatment.
When imaging or tests are needed
Imaging (X-ray, MRI) is reserved for suspected fractures, infection, malignancy, or when symptoms fail to respond to appropriate conservative care. Red flags include unexplained fever, severe localized bone tenderness, neurologic deficit, or history of cancer.
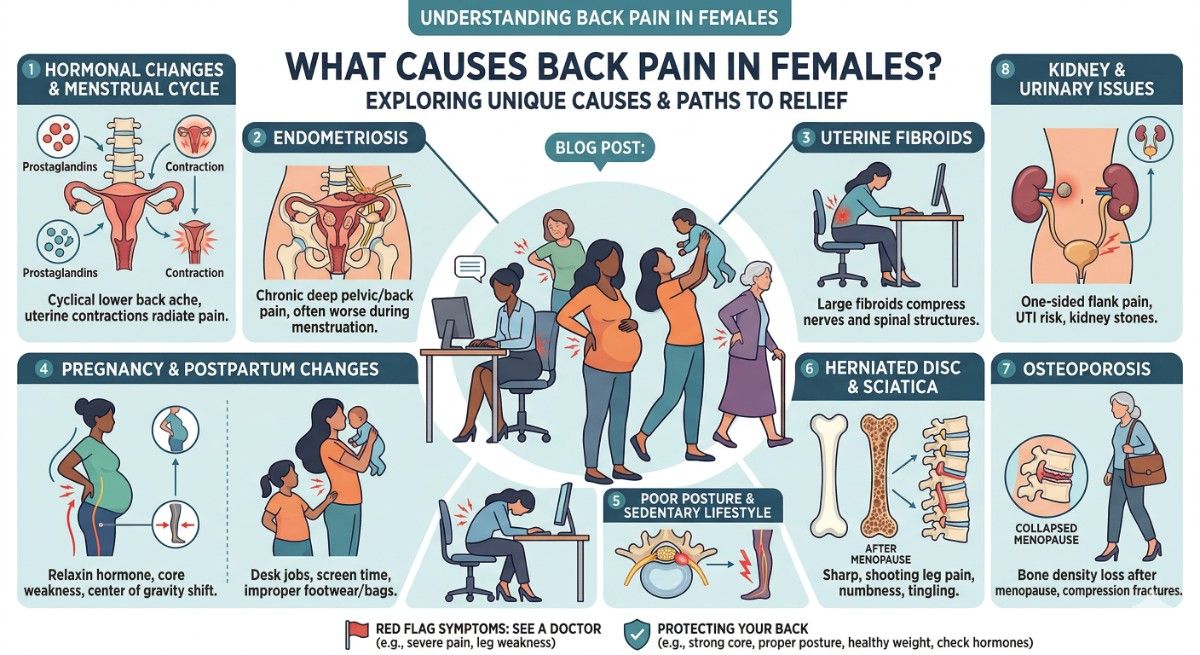
Common causes and risk factors
- Pregnancy-related pelvic girdle pain: hormonal changes and altered biomechanics commonly trigger symptoms in pregnancy and the postpartum period.
- Trauma or sudden load to the pelvis.
- Repetitive strain from occupational or athletic activities.
- Previous pelvic surgery or lumbar spine issues that change loading patterns.
Management framework: PELVIC CARE Checklist
Use the named checklist below to organize assessment and treatment. This provides a consistent, practical approach for most cases.
- P—Posture and movement analysis: correct harmful positions and teach safer movement patterns.
- E—Education: pain mechanisms, pacing, realistic recovery goals.
- L—Load management: graded return to activities, reduce provocative loads.
- V—Visits to a qualified therapist: physiotherapy for exercise prescription and manual techniques.
- I—Ice/heat and short-term analgesia: for symptom control.
- C—Compression and supports: pelvic belts can help during flare-ups and pregnancy.
Conservative treatments and self-care
Start with conservative strategies that focus on function and gradual progression:
- Targeted exercises for pelvic stability and hip strength; avoid movements that reproduce sharp pain.
- Activity modification—short, frequent walks rather than prolonged standing; sit-to-stand technique training.
- Pain control with ice, heat, or short courses of analgesics as advised by a clinician.
- Consider a pelvic support belt during activities that provoke symptoms, especially in pregnancy.
Pelvic girdle pain in pregnancy
Pregnancy-specific pelvic girdle pain is common and often improves postpartum. Management emphasizes tailored exercise, posture support, and pain coping strategies. For authoritative advice on pregnancy-related care and red flags, refer to NHS guidance.
When to refer and advanced options
- Refer to physiotherapy for persistent functional limitation or if simple self-care fails after 4–6 weeks.
- Pain not responding to conservative care may benefit from multidisciplinary review (physiotherapy, pain medicine, obstetrics if pregnant, orthopedics where structural issues are suspected).
- Interventions such as injections to the sacroiliac joint, radiofrequency ablation, or surgery are uncommon and reserved for selected, well-assessed cases.
Practical tips (actionable)
- Keep activity varied: alternate standing with seated tasks and avoid long, uninterrupted standing or stair-heavy chores.
- Use a pelvic support belt for short-term tasks that provoke pain—tighten it for lifting or long walks, but avoid constant wear to prevent muscle reliance.
- Practice a daily 10–15 minute targeted exercise sequence focusing on deep core activation and hip abductor strength under therapist guidance.
- Plan tasks in blocks to reduce repetitive bending: bring laundry baskets to waist height, sit for dressing when possible.
Common mistakes and trade-offs
Common mistakes
- Over-resting: prolonged inactivity can weaken stabilizing muscles and worsen recovery time.
- Ignoring movement quality: continuing the same movement patterns that provoke pain delays improvement.
- Relying solely on passive treatments: manual therapy or injections may help but should be paired with active rehabilitation.
Trade-offs to consider
Short-term pain relief from medications or injections can facilitate participation in rehabilitation, but these should not replace active exercise and load management. Pelvic belts can reduce symptoms during tasks but may reduce muscle activation if used continuously. Weigh immediate symptom control against long-term motor control recovery.
Short real-world example
Scenario: A 32-year-old third-trimester pregnant person reports sharp pain over the front pelvis when rolling in bed and pain in the buttock when walking. Plan: teach rolling and log-roll techniques, fit a pelvic support belt for longer walks, start a gentle home exercise program for pelvic floor and hip stabilizers, and schedule physiotherapy. Symptoms reduced within 4–6 weeks and function improved by postpartum follow-up.
Core cluster questions for related content
- What exercises reduce pelvic girdle pain and improve pelvic stability?
- How does pelvic girdle pain differ from lumbar spine pain?
- When should someone with pelvic girdle pain see a physiotherapist or specialist?
- What role do pelvic support belts and braces play in managing pelvic girdle pain?
- How does pregnancy change the assessment and treatment of pelvic girdle pain?
Key takeaways
pelvic girdle pain is often manageable with education, load management, and targeted exercise. Early, active rehabilitation improves outcomes. Use a structured checklist like the PELVIC CARE Checklist to make assessment and treatment systematic. Seek professional care if symptoms are severe, progressive, or associated with red flags.
FAQ
What causes pelvic girdle pain?
Causes include mechanical strain on the sacroiliac joints or pubic symphysis, ligament laxity (often hormonally mediated during pregnancy), trauma, and altered movement patterns from lumbar or hip problems. Many cases are multifactorial.
Can pelvic girdle pain resolve on its own?
Yes, many cases improve over weeks to months with conservative care. Active rehabilitation accelerates recovery. Persistent symptoms merit reassessment and possibly specialist referral.
Are there safe exercises during pregnancy for pelvic girdle pain?
Yes. Low-impact, supervised exercises that strengthen the pelvic floor, deep core, and hip abductors are safe and effective. Avoid activities that reproduce sharp pain and seek guidance from a physiotherapist trained in perinatal care.
How long does recovery usually take?
Recovery varies: some improve in weeks, others take several months. Consistent, progressive rehabilitation and activity modification shorten recovery compared with uncontrolled rest.
When should someone with pelvic girdle pain seek emergency care?
Emergency evaluation is needed for signs of infection, severe unexplained neurological deficits, recent major trauma, or symptoms suggesting a fracture or other acute pathology. Otherwise, routine referral to primary care or physiotherapy is appropriate.