Best Piles Treatment in Chennai 2026: Surgeon vs IR Specialist
-

- May 19th, 2026
- 3,711 views

FREE SEO Topical Map Generator: Find Your Next Content Ideas
Piles are more common than most people admit — and far more treatable than most people realise. The real problem is not the condition itself, but the silence around it. Many people delay treatment out of embarrassment and continue relying on creams, painkillers, or home remedies for months or even years.
Today, the best treatment option is not always surgery. A modern minimally invasive procedure called Haemorrhoidal Artery Embolization (HAE) is now available, yet many patients are still unaware of it. This article compares both treatment approaches, explains the difference between surgical and non-surgical care, and helps you choose the right option for long-term relief from piles. If you are searching for haemorrhoid treatment Chennai, understanding these newer treatment options can help you make a more confident decision.
What are piles?
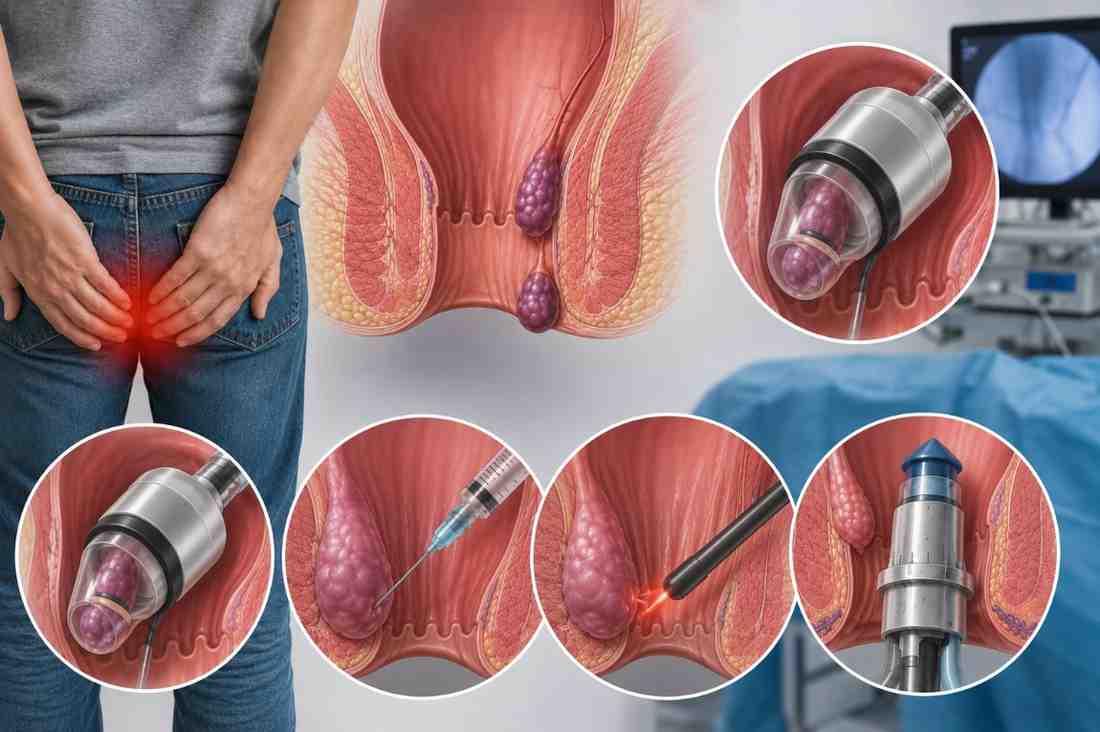
Piles, also called haemorrhoids, are swollen veins in and around the rectum and anus. They cause bleeding, pain, itching, and discomfort. They are graded from Grade 1 (internal, no prolapse) to Grade 4 (permanently prolapsed and cannot be pushed back).
Why So Many People in Chennai Wait Too Long
Most people with piles do not see a doctor. They feel embarrassed. So they treat the symptoms themselves, and the condition quietly gets worse.
The Indian Journal of Gastroenterology (2023) reports that 75% of people will experience symptomatic haemorrhoids at some point in their lives. In urban India, delayed treatment means many cases progress from Grade 1 to Grade 3 before anyone takes action.
Creams and painkillers only mask the surface. They do not treat the underlying vascular problem driving the haemorrhoid.
Symptoms people ignore for too long:
- Bright red bleeding during or after passing stool
- Pain or burning sensation around the anus
- Itching or mucus discharge
- A lump or swelling near the anus
- A feeling that the bowel has not fully emptied
Common mistake: Self-diagnosing rectal bleeding as piles without getting a proper examination. Bright red bleeding is usually haemorrhoidal, but it can occasionally indicate something more serious. Always get a clinical evaluation first, especially if bleeding is new or getting worse.
Pro Tip: If you notice rectal bleeding for the first time, do not diagnose yourself. See a doctor and get it confirmed. One quick examination gives you clarity and rules out anything that needs urgent attention.
Key Takeaway: Delayed care turns a manageable Grade 1 or Grade 2 condition into something that needs more complex treatment. The earlier you act, the simpler the solution.
Surgeon vs IR Specialist: What Each One Offers
A colorectal surgeon treats piles through surgical and procedural techniques. An interventional radiologist uses image-guided, catheter-based methods — no surgical cuts, no general anaesthesia, same-day discharge.
Most patients in Chennai only know about the surgical route. The IR pathway is rarely mentioned unless you specifically ask.
Clear comparison of both options:
|
Feature |
Colorectal Surgeon |
Interventional Radiologist |
|
Treatment type |
Banding, sclerotherapy, surgery |
Haemorrhoidal Artery Embolization (HAE) |
|
Anaesthesia |
Local, spinal, or general |
Local only |
|
Hospital stay |
Same day to 2 nights |
|
|
Recovery time |
1–4 weeks |
2–5 days |
|
Best for |
Grade 3–4 prolapsed haemorrhoids |
Grade 2–3 bleeding haemorrhoids |
|
Post-procedure pain |
Moderate to significant |
Mild |
Neither option is universally better. The right choice depends on your grade and your symptoms.
Pro Tip: Before your first specialist appointment, ask your GP to confirm your haemorrhoid grade. Knowing whether you are Grade 2 or Grade 4 shapes every treatment conversation that follows. Without that information, you are making decisions with an incomplete picture.
Key Takeaway: Surgeons and IR specialists treat piles through entirely different approaches. Knowing your grade is the first step toward choosing the right one.
What HAE Is And How It Works
HAE achieves the same goal as surgery, reducing haemorrhoidal tissue, but through a completely different route. No incision. No general anaesthesia. No overnight stay.
The procedure is performed by an interventional radiologist using live X-ray guidance throughout.
How HAE works step by step:
- Pre-procedure assessment:- Clinical examination and imaging review
- Local anaesthesia:- Applied at the wrist or groin entry point
- Catheter insertion:- A thin tube enters through a 2mm skin puncture
- Navigation to haemorrhoidal arteries — Live X-ray guides the catheter precisely into position
- Coil or particle placement:- Blood flow to the swollen haemorrhoidal tissue is reduced
- Catheter removed:- No stitches required. A small dressing is applied
- Walk out the same day:- Most patients are discharged within a few hours
A 2023 systematic review in Techniques in Coloproctology found that HAE achieved significant bleeding reduction in 80–85% of patients with Grade 2–3 haemorrhoids. Post-procedure pain was markedly lower than that of surgical alternatives.
HAE vs Haemorrhoidectomy:
|
Feature |
HAE |
Haemorrhoidectomy |
|
Anaesthesia |
Local |
General or spinal |
|
Hospital stay |
Same day |
1–2 nights |
|
Recovery |
2–5 days |
2–4 weeks |
|
Pain after |
Mild |
Significant |
|
Best for |
Grade 2–3 bleeding |
Grade 3–4 prolapsed |
Pro Tip:
Key Takeaway: HAE is a proven, same-day option for Grade 2–3 bleeding haemorrhoids. It reduces symptoms without surgery and avoids the painful recovery that follows haemorrhoidectomy.
How Chennai Patients Are Choosing Between the Two
In practice, the treatment a patient receives often depends on which specialist they see first — not which option suits them best.
Most patients go to a general physician, who refers them to a colorectal surgeon. The surgeon offers banding, sclerotherapy, or haemorrhoidectomy. These are all appropriate treatments. But HAE is rarely mentioned because it falls under interventional radiology — a different department entirely.
This referral gap means many patients in Chennai go through surgery without ever knowing a less invasive alternative existed.
Specialists like Dr Ravindran, an Endovascular and Interventional Radiologist at irdoctor Evaluate patients with piles using clinical grading and imaging before recommending any intervention. This structured, imaging-first approach means the treatment is matched to the patient's actual condition — not simply to the procedures available in one department.
For Grade 2–3 patients in particular, this distinction matters. A patient who qualifies for HAE but instead undergoes haemorrhoidectomy faces two to four weeks of significant post-operative pain, widely known as one of the most uncomfortable recoveries in routine surgical practice.
Pro Tip: If a surgeon recommends haemorrhoidectomy for Grade 2–3 bleeding haemorrhoids, ask directly: "Have you considered HAE for my case — and why or why not?" A confident surgeon will give you a clear clinical answer. A vague response is reason enough to seek a second opinion from an IR specialist.
Key Takeaway: The treatment you receive often reflects who you saw first. Knowing HAE exists puts you in a position to ask the right question before committing to anything.
Which Treatment Matches Your Grade: A Practical Guide
Treatment for piles should always be matched to the grade. This is the clearest way to avoid both under-treatment and over-treatment.
Grade-by-grade treatment guide:
|
Grade |
What It Means |
Best Treatment Options |
|
Grade 1 |
Internal only, bleeding but no prolapse |
Dietary changes, fibre, topical treatment |
|
Grade 2 |
Prolapses during straining, returns on its own |
Rubber band ligation, sclerotherapy, HAE |
|
Grade 3 |
Prolapse needs manual replacement |
HAE, rubber band ligation, or surgery |
|
Grade 4 |
Permanently prolapsed, cannot be replaced |
Haemorrhoidectomy surgery indicated |
- Rubber band ligation:- Cuts off the blood supply to the haemorrhoid. Effective for Grades 1–2
- Sclerotherapy:- Chemical injection shrinks the haemorrhoid. Best for Grade 1–2
- HAE:- Catheter-based, image-guided. Best for Grade 2–3 bleeding resistant to other treatments
Surgical options:
- Stapled haemorrhoidopexy:- Less painful than conventional surgery. Suitable for Grade 3. Recovery around one to two weeks
- Haemorrhoidectomy:- Most definitive option. Best for Grade 3–4 prolapsed haemorrhoids. Recovery two to four weeks
Regardless of which treatment you choose, do not skip lifestyle changes. A high-fibre diet, good hydration, and avoiding straining during bowel movements reduce recurrence rates for every treatment on this list.
Pro Tip: Dietary changes alone can resolve Grade 1 haemorrhoids completely. Even for higher grades, lifestyle adjustments reduce the load on treated tissue and lower the chance of recurrence. Treatment and lifestyle work together, not as alternatives to each other.
Key Takeaway: Grading drives treatment. Knowing your grade gives you a framework to evaluate every recommendation you receive — and the confidence to ask the right questions.
When to Seek Emergency Care: Do Not Wait
Most piles cases can be managed with a planned appointment. But some situations need urgent attention, same day or emergency, not a routine booking.
Go to the doctor immediately if you have:
- Heavy rectal bleeding that does not stop
- A prolapsed haemorrhoid that cannot be pushed back in and is severely painful
- Significant swelling with discolouration of the tissue, which may indicate strangulation
- Suddenly, severe pain around the anus with fever
These are signs of acute haemorrhoidal crisis or thrombosis. They require an emergency assessment, not a scheduled consultation next week.
Pro Tip: Haemorrhoidal strangulation — where the blood supply to the prolapsed tissue is cut off is a medical emergency. If the tissue around the anus looks dark, feels very hard, and is extremely painful, do not drive yourself to a clinic. Go to an emergency department.
Key Takeaway: Most pile cases are not emergencies. But some are. Knowing the difference could prevent serious complications.
FAQ: People Also Ask About Piles Treatment in Chennai
How do I know if I need surgery or a
non-surgical treatment for piles?
Your haemorrhoid grade determines this. Grade
1–2 almost always responds to non-surgical options. Grade 3 can go either way
depending on symptoms. Grade 4 with permanent prolapse typically needs surgery.
A clinical examination confirms your grade and guides the decision. Do not skip
this step — treatment without grading is guesswork.
What is HAE, and how is it different from piles
surgery?
HAE is a catheter-based procedure where an interventional radiologist
reduces blood flow to swollen haemorrhoidal vessels — without any surgical
incision or general anaesthesia. Surgery physically removes or repositions the
tissue. HAE is same-day, causes minimal post-procedure pain, and suits Grade
2–3 bleeding haemorrhoids. Surgery remains more effective for prolapsed Grade
3–4 cases.
Why is haemorrhoidectomy so painful compared
to other treatments?
The anal region has a very dense nerve supply, making haemorrhoidectomy one of the most uncomfortable surgical recoveries in
routine practice. Post-operative pain can last two to four weeks. This is
exactly why alternatives like rubber band ligation, HAE, and stapled
haemorrhoidopexy are preferred whenever clinically appropriate.
When should I see a doctor urgently for symptoms of piles?
Go immediately if you have heavy rectal
bleeding that does not stop, a prolapsed haemorrhoid that cannot be pushed back
and is extremely painful, or if the tissue around the anus is discoloured and
swollen. These are signs of haemorrhoidal crisis or strangulation, both of which require emergency care, not a routine appointment.
Which pile treatment has the fastest recovery
in Chennai?
HAE offers the fastest recovery; most
patients return to normal activity within two to five days. Rubber band
ligation and sclerotherapy are similarly quick for Grade 1–2. Haemorrhoidectomy
has the longest recovery at two to four weeks. Stapled haemorrhoidopexy sits in
between one and two weeks. Always balance recovery speed against which
treatment actually fits your grade.
Conclusion: The Right Treatment Starts With Knowing Your Grade
Piles do not have to mean weeks of painful surgical recovery. They do not have to mean permanent discomfort either.
The right treatment simply depends on your grade and whether you have been given the full picture of what is available.
Here is the simple version:
- Grade 1–2 - Start with banding, sclerotherapy, or dietary changes
- Grade 2–3 with bleeding - Explore HAE before committing to surgery
- Grade 3–4 with prolapse - Surgical assessment is the right next step
- Not sure of your grade - Get a clinical examination this week, not next month
If you are in Chennai and managing piles with creams alone, it is time to take the next step. One conversation with the right specialist — surgeon or interventional radiologist gives you a clear picture of where you stand and what to do about it.
The sooner you know your grade, the simpler your options tend to be.